
Dr. Suzuki Blog. #1
Running Q&A #1 - Keep Moving!
Posted On: Aug 2, 2021 | Posted By: Dr. Suzuki
Dr. Suzuki - Running Q&A #1 - “Keep moving!”
Question: I am training for my first marathon, but my friends are telling me I should stop running because marathon will ruin my joints forever. Is that true?
Not true! You should be staying active for your health, and marathon running is a wonderful sport for your health. As long as you are not currently injured, you should be waking and running as much as you can. “Marathon will damage your joints” is a big lie. We know that weight bearing exercises like walking/running only strengthen the joint units (including muscle/ligaments/cartilages) and PROTECTIVE of your joints in lower extremities.
The current recommendation within the US medical community is as follows: We recommend weekly minimum 150 minutes of moderate exercise (brisk walking), or minimum 75 minutes of vigorous exercise (jogging). We actually suggest you exceed those minutes, as we have enough medical evidence that the more you move, the healthier you would become. (1)
Here is one of the latest studies published by NIH in 2020 (Saint-Maurice et al. JAMA 2020). They gave accelerometers (like a Fitbit) to almost 5000 people and tracked their steps and how they did for 10 years. The results were pretty clear; if you were sedentary, you didn’t do so well (more death, in all cause mortality), while the more active you were, you were less likely to die. (2)
A separate study published by Harvard Medical School in 2019 (Lee et al, JAMA 2019) also gave accelerometers for 18,000 women and found basically the same thing; as little as 4,400 steps a day was beneficial to keep you healthy and make you live longer, while the more steps taken were more beneficial. (3)
Interestingly, both of these two studies did not find “step intensity” to be a factor in positive health benefits, meaning the walkers did as well as the runners. Big thumbs up to the walkers & the walking/running groups!
There are many more studies indicating the same results already published in Japan, where they invented and marketed a pedometer or “Manpo-kei (10000 step counter)” in 1965, after the FIRST Tokyo Olympic in 1964.
The bottom line: We often talk about “Motion is lotion” and “health is wealth” in our medical community, and for a good reason. I suggest that you keep running/walking and complete that marathon goal. I’ve completed over a dozen marathons, and I love everything about it — training, camaraderie, the sense of accomplishment — and I keep coming back. You are doing a wonderful thing for your health, and the latest medical evidence backs you up on that point.
References:
- Physical Activity Guidelines for Americans 2018, US Dept of Health and Human Services.
- Saint-Maurice et al, Association of Daily Step Count and Step Intensity with Mortality Among US Adults. JAMA 2020.
- Lee et al. Association of Step Volume and Intensity with All-Cause Mortality in Older Women. JAMA 2019.
Dr. Suzuki is a Boston marathon qualifier/finisher and an Ironman finisher. He is a foot and ankle surgeon, an attending staff of the Cedars-Sinai Medical Center. He welcomes your running or health-related questions via email (Kazu.Suzuki@cshs.org), which may be featured in our weekly emails and in our website.
(Disclaimer: This article is for your information only; it is NOT meant to be a substitute for a proper diagnosis and medical care by your own doctor.)
Have an inspired workout!
Regards,
Los Angeles Running Club
.
Dr. Suzuki Blog #2
Dr. Suzuki Blog #2
Managing Your Heel Pain
Posted On: Aug 11, 2021 | Posted By: Dr. Suzuki
DR. SUZUKI’S BLOG
Managing your heel pain
Question: I am increasing my weekly mileage in my marathon training, but now I have heel pain when I run. What do I do?
Heel pain for runners and walkers are incredibly common; I had it on and off for several years myself. Most likely, you have a condition called “Plantar fasciitis,” which is THE most common foot injury we see. Although there is such thing as a stress fracture of heel bone (calcaneus), that is a rare condition to happen, unless you are a high-mileage runner with 100+ miles per week, or you just completed an ultra marathon.
Plantar fascia is a band of ligamentous tissue that connects your calf muscles to your heel bone, and it eventually connects to the ball of your foot (see image). This is a “Pulley” system to propels you forward when you walk and run. Out of the entire foot and leg system, the plantar fascia attachment to the bottom of your heel bone is often the weakest point; hence an overuse can lead to the inflammation (—itis) of your plantar fascia (= fasciitis), causing pain.

There are many things you can do; Let me list them one by one.
1. Stretch: stretching out your calf muscles diligently will take stress off your plantar fascia and it is highly encouraged. There are a device called night splints that you wear in bed to stretch out your calves, although I don’t recommend them right away as they may be uncomfortable to wear in bed.
2. Shoes: review your running/walking shoes. Are they worn out? I see many running injuries caused by worn-out shoes, and the injuries go away gradually when you get new shoes. Are your shoes supportive enough for your activity and for your weight? I recommend enough protection and cushioning for your feet if you are a road runner/walker, based on your weekly mileage and body weight.
3. Mobilization: Remember, “Motion is lotion.” As long as your heel pain is controlled, you should be waking/running/biking/swimming as much as you can. Strengthening your foot and leg muscles would only help your cause. Cross-training with less impactful exercise (swimming and biking, even elliptical machine may work) is always encouraged when you have running injuries.
4. In-home physical therapy: Among many modalities that you could try to manage pain, I am a big fan of TENS unit (about $30 on Amazon, pictured), which is a non-drug method to increase blood flow, massage and reset the nerve signals that conducts pain sensation. RICE (Rest, Ice, Compression, Elevation) is also a simple method to alleviate acute running injuries and inflammation. We usually recommend icing the painful area, 20 minutes on & 20 minutes off, and be careful of developing frost bite (perhaps, don’t sleep with ice on).
5. Over the counter topical medication: Topical pain creams including voltaren gel (diclofenac), salonpaas (menthol), Lidoderm patch (lidocaine) and various CBD creams. They all work differently and one of them is bound to work well for you. Quick tip: Voltaren gel is very effective for knee and ankle and foot pain and it’s now generic and much cheaper now, about $20 per tube.
6. Over the counter oral medications for pain: I usually recommend starting with over-the-counter acetaminophen (Tylenol) 500-1000mg around the clock (every 6 hours, or at each meal plus bedtime), You can take up to 4000mg per day of Tylenol safely. That’s two extra strength Tylenol 4 times a day. I shy away from recommending NSAIDs — ibuprofen (Advil), naproxen (Aleve), Diclofenac (Voltaren) etc — due to concern of GI bleeding and kidney stress, but it is probably safe if you limit it for two weeks or occasional use.
7. Weight control: This is all about physics, not vanity!! If you have excess weight to lose, just losing 5-10 pounds may make a world of difference in your foot and ankle pain, as you exert 2-5 times the amount of body weight to your feet when you run. For weight control, I am a big proponent of plant based diet (I’m a vegan), I practice 16-8 hour time-restricted eating methods (also called intermittent fasting). I have been following a (relatively) low-carb diet, after checking my diet with a continuous glucose monitor for 4 weeks. I recommend USC’s ProLon diet (fasting mimicking diet) program when my patients want to lose weight for their health reasons.
8. Seek help from a medical professional: Lastly, if your heel pain persists more than two weeks, it’s probably time to seek a medical professional help. Podiatrists (foot and ankle doctors) or orthopedists can help you in making the diagnosis of plantar fasciitis, rule out stress fracture (you may need X-ray and MRI imaging for that) and coming up with the treatment plan. My treatment for you would include all of the above, plus prescription medication as needed, as well as injection of corticosteroids (Kenalog), which is VERY effective in calming down the inflammation and pain. I find that a series of 1-2 heel injections often make the heel pain go away and get you back into running/walking activities. In addition, I may write you a prescription to go see a physical therapist; they can help you in guiding you through various stretches and apply physical therapy treatments. There are many “newer” heel pain treatments like shockwave therapy and botox injections, but I don’t recommend them as I haven’t seen convincing medical evidence for them

Dr. Suzuki is a Boston marathon qualifier/finisher and an Ironman finisher. He is a foot and ankle surgeon, an attending staff of the Cedars-Sinai Medical Center. He welcomes your running or health-related questions via email (Kazu.Suzuki@cshs.org), which may be featured in our weekly emails and in our website.
(Disclaimer: This article is for your information only; it is NOT meant to be a substitute for a proper diagnosis and medical care by your own doctor.)
Have an inspired workout!
Regards,
Los Angeles Running Club
Dr. Suzuki Blog #3
Dr. Suzuki Running Blog #3: Runners Guide For COVID-19 Prevention
Posted On: Aug 18, 2021 | Posted By: Dr. Suziki
Dr. Suzuki Running Blog #3: Runners guide for COVID-19 prevention
Dr. Suzuki is a Covid-designated physician & He can answer your COVID related questions. He will be bringing fun-colored masks to the totem pole and to the track nights to be given away.
Q. I heard Covid-19 numbers are up again in the hospital. Is that true?
Yes it’s true. In early July 2021, Covid patients in our hospital were down to a few patients. Now we are closer to 100. We are staring to cancel elective (non urgent) surgeries to save our beds and resources. Now, we also require the visitors and the hospital workers to show the proof of vaccination.
Q. I didn’t get around to get the COVID vaccine. Should I still get one? Is it really safe?
Yes. Covid vaccines are very safe and very effective. As of last week, about 197 million Americans have received at least one dose of a Covid-19 vaccine, including about 167.7 million people who have been fully vaccinated by Johnson & Johnson’s single-dose vaccine or the two-dose series made by Pfizer and Moderna. About 71.6 percent of adults in the US have received at least one shot.
As for its safety, FDA is about to give Pfizer vaccine a full approval for its safety and efficacy, anytime between now and early September. The ingredients of vaccines are quite simple, mRNA (virus spike protein) and the absorbable container, which is made of lipids (PEGs, as in toothpaste), salts (as in table salt) and sugar (Sucrose). Note that you CANNOT get COVID from the vaccine itself, as it does not contain the actual virus.
The vaccine teaches our immune system what to watch out for, so that when your body recognize the virus, it attacks the virus right away, preventing infection in most cases, and preventing severe disease (and hospitalization and death) in over 99% of cases.
Q. But you can get infected even after full vaccination? Then what’s the point?
Yes, but that’s rare and It’s called breakthrough infections. First, the vaccines can prevent infection, but more importantly the vaccines prevent severe disease and death, and it’s really good at that.
Let me show you two recent real-life cases in July 2021:
1. Fourth of July event in Provincetown MA: this was a huge annual event with 60,000 people gathering and partying up. It was a rainy weekend, and it created many indoor gathering situations and a cluster of infections. The results were 965 COVID infections… but resulted in 7 hospitalization and no death.
2. San Francisco General and UCSF hospitals in July: we recently had a mini outbreak in the hospital in downtown SF… which resulted in 183 infection, two hospitalizations and no death.
The common thread here, was 3/4 of these people were vaccinated and well protected. The full vaccination renders COVID (fairly) harmless, bringing the rates down to 0.004% of hospitalization and 0.001% of death recorded by CDC. This is much less deadly than seasonal flu numbers.
Q. I already had a covid infection. I don’t need a vaccine right?
Yes you do. We have been checking the antibodies of previously infection people, and their antibody levels may be unreliable. The current guideline is to give a vaccine to previously infected people, which resulted in super high antibodies to protect you, even higher than two vaccines and no previous infection.
Q. Are we ever going to be done with COVID pandemic?
As the virus spread from person to person, it continues to replicate and mutates. Unfortunately, Covid virus isn’t going away completely and we expect it to be endemic; meaning we have to learn to live with it, just like flu or cold. I grew up in Tokyo Japan, where many people wear masks routinely during winter (flu/cold season) and spring (hey fever season). I can see it being the new habit here in Los Angeles to keep you safe from COVID, flu and cold.
Q. I’m fully vaccinated now. What’s going on with the booster shot?
As of now, if you are immune-compromised, such as transplant or cancer patients, you CAN get a third shot of vaccine. You do NOT need a doctor’s note, It’s an honor system; you just have to attest that you are at risk and benefit from that third shot. If you are healthy, you don’t need a booster shot yet.
Q. Is it safe for us to be running together?
YES. If you are fully vaccinated, it is considered safe to be running outdoor with others. I still recommend that you wear a mask indoors, like grocery stores or shopping malls. If you are still unvaccinated, I highly recommend that you get that shot. It’s safe, effective, it saves your life, and it prevents your friends and family from catching the virus. Thank you!! —> www.vaccines.gov
(Sources: CDC.gov, New York Times)
Dr. Suzuki is a Boston marathon qualifier/finisher and an Ironman finisher. He is a foot and ankle surgeon, an attending staff of the Cedars-Sinai Medical Center. He welcomes your running or health-related questions via email (Kazu.Suzuki@cshs.org), which may be featured in our weekly emails and in our website.
(Disclaimer: This article is for your information only; it is NOT meant to be a substitute for a proper diagnosis and medical care by your own doctor.)
Have an inspired workout!
Regards,
Los Angeles Running Club
Dr. Suzuki Blog #4
Blog #4 More Update On COVID Infection And Vaccine Boosters
Posted On: Aug 25, 2021 | Posted By: Dr. Suzuki
DR. SUZUKI’S BLOG
More updates on COVID and vaccine boosters”
Dr. Suzuki is a Covid19-designated physician & He can answer your COVID related questions. He will be bringing fun-colored masks to the totem pole and to the track nights to be given away to the club members.
Q. What’s the state of COVID infection in LA county right now?
In LA county, our vaccination rate is 65% (at least one dose) and we are averaging 33 new cases per 100,000 residents. In brief, we would like you to be careful and take all the prevention measures, but we are doing okay compared to the other struggling states, due to our higher vaccination rates.
The COVID infection number is worse than in it was in June, but it is no where near the peak, around the last Xmas when we had 180 new cases per 100,000 people. Our 7 day average infection rate is 1.03 — so it is still spreading slowly in Los Angeles. Our hospitalized patient numbers have been holding steady for the last two weeks and the vast majority (99%) of our COVID patients in the hospital are unvaccinated people.
Q. What’s the deal with FDA full-approval of the vaccines?
It is reported that FDA is going to grant a full authorization of Pfeizer vaccine this week, meaning that after weighing all the data based on over 200 million doses given, FDA determined that Pfeizer vaccine is SAFE and EFFECTIVE against preventing COVID19 infection and complications, and it will be endorsed just like any other vaccines for flu, shingles, polio and others.
Q. What about this booster vaccine shot? Should I get one now?
For certain individuals with compromised immune system, we recommend that they make an appointment and receive a third shot right now. Examples are; people with cancer treatment or transplant patients, or active treatment with steroids or other immune suppressing medications. FYI, you do NOT need a doctors note to get a third vaccine shot, as it is self-attestation basis. Now you can make an appointment specifically as a third shot.
For the rest of us, with healthy immune function, CDC will recommend a 3rd shot of mRNA vaccines (Pferzer and Moderma) as it will boost the antibody level by at least ten-fold. It is recommended that you get the same vaccine as the previous 2 shots, starting on September 20th and ideally before the winter season, when we can expect another surge in COVID cases.
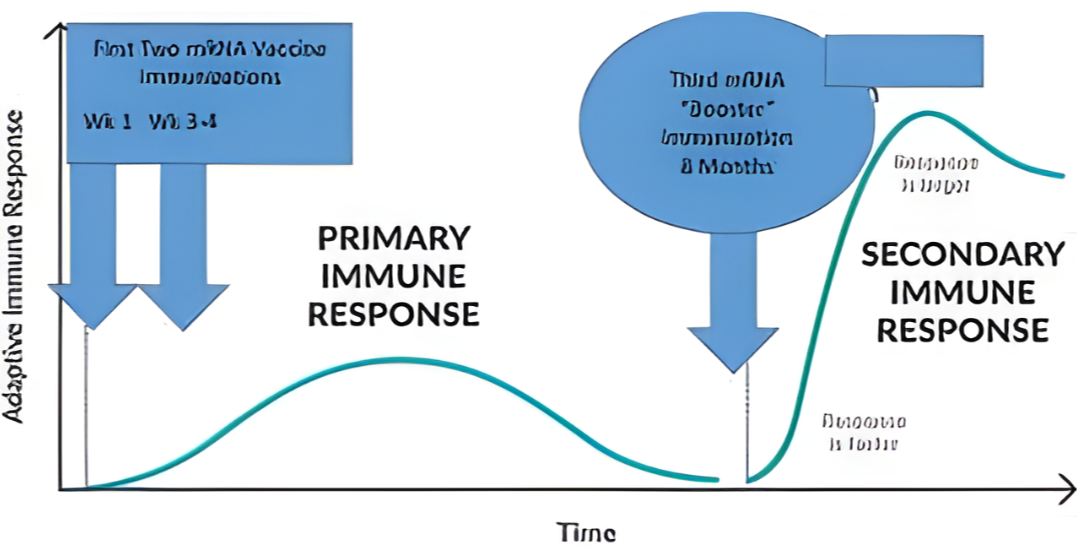
Q. Does this mean we have to get a shot every 8 months?
We don’t have the data on that, but it’s unlikely. Many vaccines (examples: Tetanus, H Flu and Polio etc) are given as a series of 3 shots, and the protections are enhanced and very long lasting after the third shot (see the illustration - source: NY times & @peterHotez MD PhD).
Q. I’ve got the one-dose Johnson & Johnson vaccine. What about me?
Since J&J vaccine was developed and introduced much later, we still don’t have enough data or formal CDC recommendation yet… but it is forthcoming. I will update you later on this blog.
Q. What about masks? Do we still need it?
Mask is an inexpensive but effective tool that protect you against the virus, as well as keeping a person from spreading the virus. In LA county, we are back with the mask mandate which will protect you and others, including large outdoor venues like Dodger stadium and Hollywood Bowl, mandating to use a mask except when you are eating and drinking at your seat.
Q. Is it safe for us to be running together?
YES. If you are fully vaccinated, it is considered safe to be running outdoor with others. I still recommend that you wear a mask indoors, like grocery stores or shopping malls, and at large venues like Dodger stadium. If you are still unvaccinated, I highly recommend that you get that shot. It’s safe, effective, it saves your life, and it prevents your friends and family from catching the virus. Thank you!! —> www.vaccines.gov And www.myturn.ca.gov
(Sources: CDC.gov, New York Times)
Dr. Suzuki is a Boston marathon qualifier/finisher and an Ironman finisher. He is a foot and ankle surgeon, an attending staff of the Cedars-Sinai Medical Center. He welcomes your running or health-related questions via email (Kazu.Suzuki@cshs.org), which may be featured in our weekly emails and in our website.
(Disclaimer: This article is for your information only; it is NOT meant to be a substitute for a proper diagnosis and medical care by your own doctor.)
Have an inspired workout!
Regards,
Los Angeles Running Club
DR. Suzuki Blog #5
DR. SUZUKI BLOG # 5 MY ADVICE ON RUNNING SHOES
Posted On: Sep 8, 2021 | Posted By: Dr. Suzuki
DR. SUZUKI BLOG “MY ADVICE ON RUNNING SHOES”
Q. I’m doing a marathon training for this fall. Which running shoes do you recommend?
I get asked about this question often! As a foot and ankle doctor with 19 years of clinical experience and examining probably close to 200,000 people, I can tell you that no two feet are exactly alike; some are narrow or wide footed, or flat to high-arched. Oftentimes, we have one foot that is bigger than the other - half size difference is not uncommon — NBA players I have worked with, obviously having gigantic feet, they can have more than one full size difference, needing to order two pairs of shoes, which they burn through in two games!
As a part of my research and curiosity, I have tried a dozen different brands of running shoes; and my best advice to you is, try several different shoes across brands and pick a pair that fit your feet the best. Do not compromise on fit. There should be zero to minimum “break-in” period, and your shoes should feel GREAT and comfortable when you put your foot down. Most shoe companies now offer wide forefoot sizing for the people with bunion issues, and “knitted” uppers (like Nike Flyknit or Adidas Primeknit) are more forgiving in fit.
For “everyday” training shoes, I recommend Nike Pegasus or Hoka Clifton as a good starting point for novice runners, as they are versatile, easily available and fairly affordable, especially if you can find the last years models. For heavier runners, Nike Vomero, Hoka Bondi, ASICS Kayano are good choices that I have worn personally and liked.
Runner’s World magazine publishes trust-worthy reviews of new shoes, and many YouTube channels do a lot of good reviews (look up “Kofuzi” and “Ginger Runner” etc). In general, you do get what you pay for, and the more expensive shoes (ie. Nike Vaporfly) tend to be lighter and FASTER (more on that below). Since running/walking is a “cheap” sport with minimal required equipment, I do suggest that you invest in shoes for your maximal running pleasure.
In terms of cushioning, I do recommend getting enough cushioning for the weekly distance that you do and based on your weight. You may not need much cushioning if you are only racing 5k, while you want more protection for your feet for marathon training with high weekly mileage. Since road running creates so much pounding on your feet, you really do need that protection to prevent foot injuries. In fact, when minimal “barefoot” running shoes became popular after Christopher McDougall’s best-seller “Born to Run” book (published in 2009), we saw a sudden increase in stress foot fracture (although we never got to publish that data). In the 2020 ESPN film, “The Infinite Race,” you see the Mexican Tarahumara runners (who run on grass fields) laughing at the Americans running barefoot in the NYC Central Park.
How about arch support? There used to be a lot of “motion control” shoes on the market, but we see less of them today. The idea of “controlling” your gait using corrective stiff shoes never made sense to me. If you have a bad running form, you should fix it with training, perhaps with your running coach, rather than correcting with your shoes. We don’t put a brace on a little league pitcher to correct their pitching form, do we?
I apply the same approach with the orthotics, either over-the-counter or prescription. Yes, if you have painful flat feet condition and a pair of orthotics alleviates the pain, that’s great; however, I have yet to see a study that athletes with normal foot type benefit from expensive orthotics. Please do invest that money back into the high quality shoes and change them often.
We say you should replace your running shoes for every 300-500 miles as the cushions bottom out; although this mileage number also varies based on your weight and shoe durability. Strava (app) can track this mileage for you, or you may want to retire your shoes once they feel “flat” and lose the “bounce.” Your running shoes are like your tooth brush, and they are not meant to be used 6 months straight. I do see that many running injuries (heel pain being the most common) may originate from using worn-out shoes. It is also recommended that you have at least two pairs of running shoes, so you can rotate them daily as they compress down and get moist from your sweat.
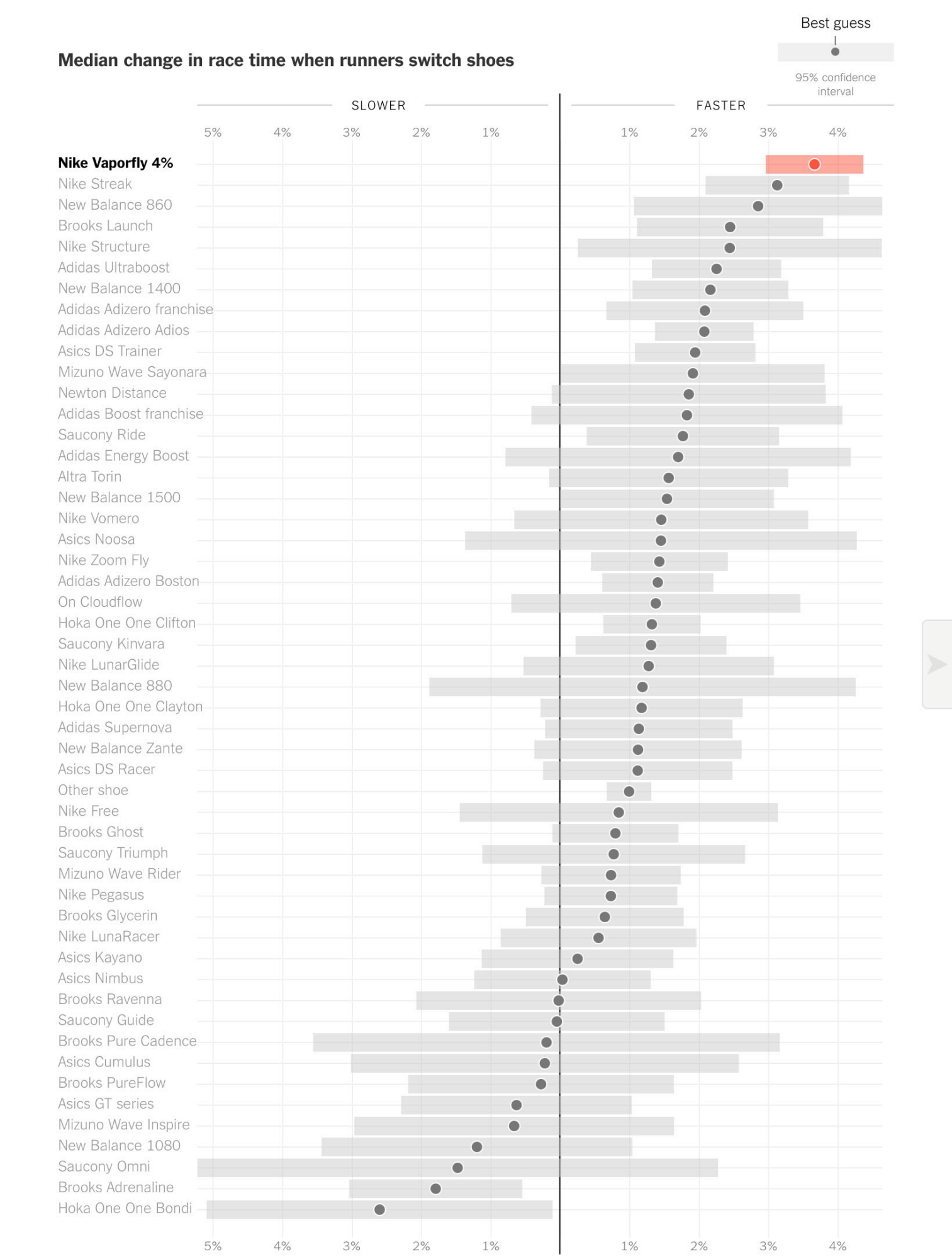
Lastly, I want to mention an interesting “racing shoe” study from New York Times (published 2018), in case you are looking for a Personal Record, or let’s say you want that Boston Marathon Qualifier time.
After analyzing the HUGE amount of Strava date from real-life races (based on 700 races with 280,000 marathons and 215,000 half-marathons completed), they found that the fastest shoes were Nike Vaporfly 4% (which contain patented curved carbon plates as leaf springs) while the slowest shoes were Hoka Bondi (which are great shoes that I recommend often, but they are maximally cushioned and very heavy).
If you look at the chart below, clearly thin and lighter “race” shoes (Nike Streak and Adidas Adios) resulted in faster race finishes, while heavier and more structured shoes were “slower,” which are NOT surprising… all the while Nike Vaporfly (the only carbon-plate shoes sold at the time) came on top.
This finding was confirmed by a 2018 Nike-funded study by University of Colorado found that Nike Vaporfly shoes were, in fact, 4% more energy efficient than conventional shoes (Nike Zoom Streak) based on 18 elite runners on treadmills. This is why these shoes were the choice of many Elite marathon runners for the last several years, including the latest Summer Olympic Games in Tokyo. (Note: most other shoe companies NOW make carbon-plated running shoes, ASICS, Adidas, HOKA, New Balance etc).
Have an inspired workout!
Regards,
Los Angeles Running Club